

An inquiry for the vaccinators: What happens when...?
An inquiry for the vaccinators: What happens when...?
Science Ignored

Although many are ready to move on from the COVID-19 “pandemic”, we are not out of the woods. The past three years have illuminated society’s manic drive for “scientific consensus” and conformity (authoritative “dead science”) compounded by an extreme bias toward the safety of medical and technological intervention, in this case an experimental therapy we labeled “mRNA vaccine” that fails to meet any prior vaccine standards—neither for safety nor efficacy. This mania and bias contribute considerable damage to our health, our communities, our information ecosystems, and our social institutions.
I previously embraced a bias of “vaccines are universally good,” deeply engrained since birth, which led to my initial acceptance and support of a wholly unusual injection that induces novel lipid nanoparticle-mRNA transfection throughout our body, bones, and organs. We call it a “COVID mRNA vaccine.”
My bias has been slowly chiseled away during the COVID years as a growing preponderance of scientific research presents evidence that is completely contrary to the regulatory and health agency talking points, mainstream journalistic stories and fact checks, and, ultimately, medical recommendations. I contend that our societal bias toward technological intervention, the “authority of science” to provide a single answer, and vaccines in particular, has enabled a near complete wiping from collective consciousness the true gravity of our situation and the pitfalls of these new therapies. Especially when they are designed around the COVID-19 spike protein antigen, which has been repeatedly demonstrated to induce many of the pathologies of COVID and is not somehow “safer” when generated via mRNA (or other) vaccination, as based on a growing body of evidence.
Our misplaced faith in COVID vaccinology (and the integrity and good will of leaders and regulators) has led global society at-large to embrace, spread, advance, and now “move on” from a series of severely disinformed actions without fully recognizing our mistakes and holding ourselves accountable to these lessons. Specifically, I’m talking about the hyper and indiscriminate COVID vaccination of all age groups, and the extreme and perverse pressure tactics many implemented to achieve this.
The result is a poorly informed populace increasingly susceptible to reinfections and with little awareness of the systemic damages introduced by both COVID and vaccination, while evidence-laden treatments (e.g., nattokinase) remain taboo or ignored.
Now banned in many civilized countries except for some rare cases among those at highest risk (older age, co-morbid), the US continues to authorize and recommend COVID vaccines and boosts for everyone, including 6-month-old infants. In fact, it's been added to the CDC childhood immunization schedule that US states require for public school, and many university and other private vaccine mandates remain in place.
I write this to spread more awareness and reflection of the unbiased and uncorrupted science and research on the mRNA technologies and other pandemic pipe dreams.
And so that we all might better work together to understand, stall, and hopefully unwind the many related and growing nodes of societal harm, like:
ongoing infant injections in the USA that have repeatedly been shown to cause a “net harm” in any risk-benefit analysis that cares to ask,
California’s deeply-misguided “medical consensus” legislation that is serving as a global model for authoritarian overreach into patient-doctor relationships, currently under court challenge with cringe-worthy state’s attorney statements to witness
fascistic new Australian censorship and information control legislation introduced to squash any dissenting views and information sources on the internet, anywhere (with convenient exemptions made for all the big state-funded and tightly-regulated news content and sources), and
attempts by WHO and medical regulators everywhere to distort scientific discourse through authoritarian “misinformation” ministries, censorship of doctors through captured licensing boards, and other significant power grabs, including literal control over what is injected into your body and your access to basic human needs.
It will likely take much more than this article to persuade one not already convinced of the corrupted pretense and pressures that led to our disinformed embrace of “COVID vaccines” and bad medicine, but I share a few breadcrumbs that connect to the bigger picture assumed in my writings, and perhaps I will unpack more of this in future work alongside the many other researchers and journalists who cover the topic extensively. But primarily, I write now to debunk any remaining support for the dangerous mRNA technology as it stands today, summer 2023, and to encourage no further voluntary injection of COVID spike protein mRNA into you and your children. Please stop with the injections.
Good medicine flows from information. As always, information is power, and it is critical people maintain transparent and uncensored information conduits across diverse perspectives in today’s biosecurity state.
Censorship and The Great Disinformation Blame Game
In hard opposition to Australian’s and California’s (and others’) explicit authoritarian policy objectives to squash opposing viewpoints and dissent, a federal court in the USA ruled July 2023 that the White House needs to back off on its extensive censorship of social media, commenting “the evidence produced thus far depicts an almost dystopian scenario,” with many medical information suppression and censorship tactics uncovered in the case, and:
the present case arguably involves the most massive attack against free speech in United States’ history
Like everything else in the USA these days, a well-evidenced case of oppressive and coordinated government censorship to maintain its own disinformation narrative is getting spun 180 degrees by the media elite, and folks are patterned to eat it up (division vs. reality). Aaron Kheriaty, a plaintiff in the case, wrote in 2022:
this evidence suggests we are uncovering the most serious, coordinated, and large-scale violation of First Amendment free speech rights by the federal government’s executive branch in U.S. history. Period, full stop. Even wartime propaganda efforts never reached this level of censorship, nor did the government in days past have the power of today’s social media at its disposal.
Aaron was former Professor of Psychiatry at the University of California at Irvine School of Medicine, where he was the director of Medical Ethics. You should hear his story as a powerful anecdote. Ethical ethicists have been forced out of their institutions. Doctors, nurses, and conscientious objectors of all types have experienced a similar fate.
In March, Matt Taibbi shared (alongside a pile of evidence of governmental overreach and deception in the #TwitterFiles) evidence of Stanford Virality Project’s censorship of “stories of true vaccine side effects” in collusion with social media firms and government—to censor those of us getting harmed by the mRNA injections, so that more people would take it.
Ends never justify the means, period, and especially censoring true information to “combat vaccine hesitancy,” as we have strong evidence to support and warrant hesitancy (anger) over the COVID-19 shots.
This sort of Stanford Virality Project-catalyzed “pro-vax” disinformation campaign was and continues to be justified by the morality of many, shaped by a myth that has been force-fed to the public through the very same disinformation efforts: namely, that IF YOU DO NOT take an experimental intervention (in this case, an injection of custom mRNA), YOU WILL KILL and HARM US.
Never mind that the wimpy clinical trials for said experimental intervention relied on flimsy and questionable positive/negative testing data, did not look at all-cause outcomes, and sold us on an alarming heap of serious adverse events. Or that folks warned the experimental intervention likely wouldn’t stop any of this. And, hmm, the vaccinated are probably prolonging the pandemic through unconstrained variant evolution in immuno-tolerant states. And they are getting sick from COVID more often and for longer, likely contributing to more spread. And so on.
Since the very “beginning” we’ve been warned to pay attention to the dangers of intervention, and censors have attempted to suppress our awareness of these dangers. The timeline is important, and I contend that there was never a moment in the past where we had uncorrupted evidence of “safety and efficacy.” See various exposes of the Moderna and Pfizer clinical trials as a starting point, including the flawed premise to use PCR positive tests as the metric of success, failure to double-blind, and vaccinating the control group after 60 days; the Jackson vs. Ventavia case (and justification for dismissal—the government was in on it, appeal pending); Michael Yeadon; Sasha Latypova analysis of the underlying US DoD “military countermeasures” OTA contracts and absence of regulatory accountabilities, and so on. But this is not my focus here.
If you’re forcing or pressuring uptake of a radically-novel medical intervention, you better have top class evidence of its all-outcome safety and efficacy (relative to the no-action alternative)—that evidence does not exist for the COVID injections, and never did. In fact, this article scratches the surface on the preponderance of damning evidence against safety and efficacy.
“Net Harm”
There are many threads to unravel and expose. What follows is some of the most critical scientific evidence and questions regarding these experimental technologies that nag at me, and that are perhaps helpful in “unlodging” any reader bias. If you doubt that the answers to these questions implicate serious concerns and legitimate propensity for widespread vaccine harm, I recommend you sit with that, focus on that. Why? Empirical big data? Released and analyzed by whom? What does it really tell you?
We know from independent, peer-reviewed analysis of the official Moderna and Pfizer phase III clinical trial data that, on average, every 1 in 800 primary series vaccinations were associated with a serious adverse event of special interest, in excess of placebo baselines. That’s hospitalization, disability, life-threatening or other medically important event, and/or death. And that’s a lot.
Please do not brush this data aside as “not causal” or use some other protective, cognitive shielding—consider with an open mind that this is quite likely a low estimate of incidence of harm. Independent, peer-reviewed evaluations of profit-motivated pharmaceutical trials are vital to help synthesize truth. Stay with me.
We have not been provided with a good study on the age distribution of adverse events (nor are researchers identifying and linking all the “events” at this point, nor looking to unvaccinated controls), which is critically important to understand. But some event classes have shown far higher rates among young as compared to old (e.g., pericarditis and myocarditis in adolescence). For example, this August 2022 study found 30% of adolescents had a “cardiac manifestation” following their second shot. Fortunately “clinical presentation was usually mild and temporary” (myocarditis is a life-long affliction, by the way, never “mild,” as you never know when that little scar might get you), and one child out of 301 (0.3%) went to the ICU. From a single “vaccine” injection. Yeah, that’s not good. In total, 1 in 150 (0.7%) children were hospitalized from a single shot.
Again, 1 in 800 is optimistic/conservative for severe adverse events—this technology damages people frequently.
The authors of the prior-referenced evaluation of clinical trial data call for formal risk-benefit analysis, and offer a conclusion that should have been made early on from the clinical trials:
In the Moderna trial, the excess risk of serious AESIs (15.1 per 10,000 participants) was higher than the risk reduction for COVID-19 hospitalization relative to the placebo group (6.4 per 10,000 participants). [3] In the Pfizer trial, the excess risk of serious AESIs (10.1 per 10,000) was higher than the risk reduction for COVID-19 hospitalization relative to the placebo group (2.3 per 10,000 participants).
For both Pfizer and Moderna trials, the excess risk of vaccination exceeded any associated COVID risk reduction.
We know the “95% efficacy” propaganda we were sold initially from the clinical trials was based on an 0.84% absolute reduction in COVID infection risk (0.88% reduced to 0.04%) during the short trial timeframe, which we now know wanes rapidly. The hospitalization and death risk reduction is some infinitesimally marginal factor of that. Remember the Aug 2022 study of 13- to 18-year-olds that found a 0.7% incidence of hospitalization (and 0.3% for ICU hospitalization) from a single Pfizer injection. Think through the magnitudes of scale here.
And I don’t want to see your charts that shows relatively more unvaccinated COVID deaths and hospitalizations—this is terribly unhelpful data, as we’ve mismanaged tallying of COVID deaths, discriminated and refused healthcare for the unvaccinated (and the many other factors between unvaccinated and vaccinated populations that must be controlled for—“healthy user bias” makes vaccines look better), and completely avoided and censored the investigation and counting of vaccine-induced disease/disability/death, including MORE COVID ITSELF.
This is why folks tend to demand long-term, double-blinded, placebo-controlled studies looking at all health outcomes. Since the vaccinators manically (deceptively) opted to vaccinate the control group in their trials just weeks after the investigations began, while systematically undercutting studies of unvaccinated cohorts, we must extrapolate whether the benefit of this novel technology comes close to “offsetting” its horrid, frequent side effects. Many have attempted; few have been heard.
Recently, the UK Health Security Agency (HSA) found that 300 people age 70 years and older would need to receive the (first) primary vaccine series to prevent one COVID hospitalization in that age group—the “number needed to vaccinate”, or NNV, is 300. The clinical trials suggest for every three (3) “avoided COVID hospitalizations” at least one (1) patient will go to hospital due to a severe adverse event from the primary series. Harm one to save three. Maybe ok?
For those younger, the situation is quite a bit worse—the UK HSA found that 11,200 kids age 16-19 would need to be injected with the primary series to prevent one COVID hospitalization (NNV of 11,200). We extrapolate from the clinical trials that 14 of these kids may end up with a severe adverse event from the initial vaccine therapy, visiting the hospital or worse. Harm 14 kids aged 16-19 to save one. Harm 42 kids aged 5-11 to save one, and so on.
Among all the folks “in a risk group” ages 20-59, the NNV ranged from 800 to 2,400. Harm one to three of those “at-risk” to save one.
The NNV for the August 2022 and Spring 2023 boosters have increased considerably for all ages.
That’s bad math for the mRNA injections. I applaud John Campbell, who has recently become an evidence-driven skeptic, for his concise video analysis of this and many other concerning data of late.
Or this peer-reviewed study with co-authors from Johns Hopkins, Harvard, Oxford, UCSF and others which used CDC NNV and clinical trial data and finds:
Booster mandates in young adults are expected to cause a net harm: per COVID-19 hospitalisation prevented, we anticipate at least 18.5 serious adverse events from mRNA vaccines.
“Net harm.” At least 18.5 serious adverse events (hospitalization, disability and/or death) for every prevented hospitalization. That is sizable net harm across the population, let alone for the individual. We see evidence for this net harm reinforced in continuous big data gathering, such as the above UK NNV statistics.
All of the foregoing is assuming the adverse event data documented in the clinical trials, which were time-limited following vaccination (e.g., Pfizer limited reporting from dose 1 to 1 month after dose 2) and excludes any potential mid- and longer-term adverse events. That’s the big empirical data.
Everyone now rightly assumes an elevated serious adverse event rate, but this continues to be propagandized by the vaccinators as “not that bad,” and, they say, “much better [or safer] than the risk of COVID.” This propaganda is found as various boilerplate in many studies and articles which themselves don’t look at the risk-benefit and despite the evidence of net harm in the studies that do. Unfortunately, the clinical trials provided ample evidence of vaccine harm, but we assumed without testing:
COVID would be worse (we must dissect each pathology to validate—the "vaccines” have some unique propensities for harm that COVID itself does not), and,
that the vaccinated would not get COVID, let alone repeatedly, and,
that “mild,” repeated COVID is benign if you are vaccinated (“risk doesn’t stack” argument).
Remember, prominent peer-reviewed research from Cleveland Clinic published April 2023 found:
The higher the number of vaccines previously received, the higher the risk of contracting COVID-19 (Figure 2).
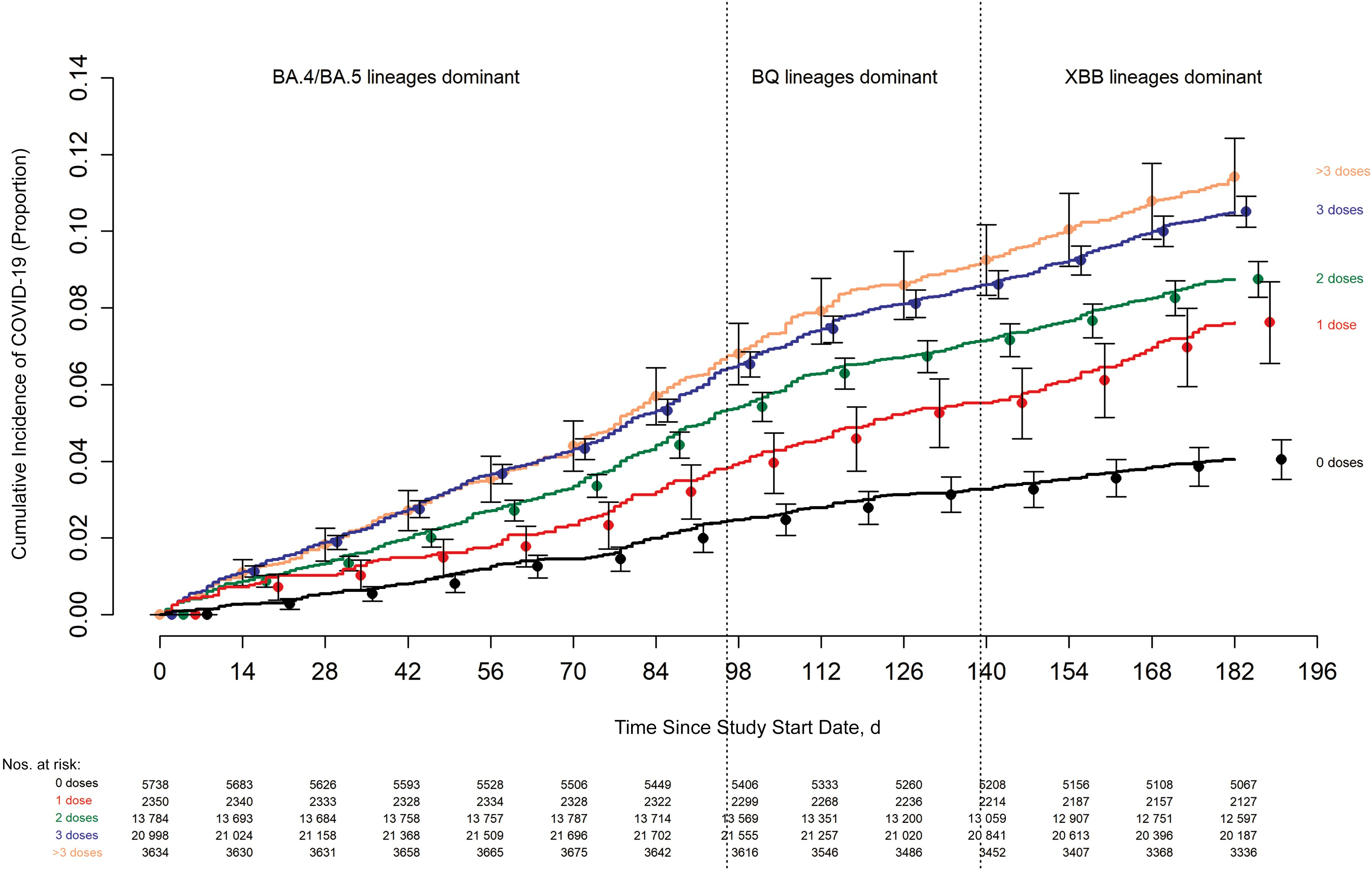
Read that again if you need to. The chart is about as simple. The authors maintain their pre-print findings, which were available in early fall 2022 for all to see, before most people took the bivalent boosts. Older studies have found the same. The vaccinated are NOT being spared the mild yet damaging repeat infections. In fact, we are getting sick more.
Studies are repeatedly showing that any vaccine efficacy that can be measured wanes promptly and into negative efficacy (see figure), while the danger from injection side effects, including susceptibility to COVID itself, appears to compound over time.

Intelligent people have warned us since…early 2020. Yet we have witnessed the “story of COVID vaccine science” to be repeatedly and intentionally obfuscated by regulators, the media, politicians, and biased advocates, including doctors and a manic and fearful populace.
You will see illuminated in the following “What happens when…” questions that the injection poses unique propensity for harm and broad shifts in our homeostasis, quite independent from (but often overlapping) COVID dynamics itself, and adverse events will plausibly occur for months and years later. This makes the bad math we can confirm today even worse. The clinical trials looked for adverse events within narrow time periods (and found alarmingly high rates), yet all the evidence suggests this new mRNA technology can have devastating side effects for as long as a lifetime.
I sprinkle citations throughout to punch holes in and debunk the dual myths of COVID vaccine “safety” and “efficacy,” but the supporting literature review is much more extensive, indeed. Scientific consensus, for what that shoddy term is worth, is most certainly not leaning toward a story of “safe and effective.”
Assuming our regulators continue to recommend and attempt to inject everyone repeatedly, experts and communicators need to urgently help society better understand and answer some question. Let’s begin:
What happens when…
…you inject the genetic code to create a foreign protein that looks like those from your own body?
The COVID spike protein shares extreme self-similarity (or molecular mimicry) with human proteins. Big parts of the spike protein look like your own body. The odds of this similarity between foreign and human protein occurring naturally are “unexpected and highly improbable.”
(This also piles onto the evidence for the lab-engineered origins of the spike protein. Pressured withdrawals of early evidence that corroborates concurrent published work of unusual spike protein inserts, alongside extensive cover-ups and discrediting and reputation wrecking, make the entire situation completely maddening and difficult to understand, but one thing is clear—the flow of information has been tightly constrained and controlled through coordinated action. But I digress.)
More technically regarding the spike protein:
A massive heptapeptide sharing exists between SARS-CoV-2 spike glycoprotein and human proteins. Such a peptide commonality is unexpected and highly improbable from a mathematical point of view, given that, as detailed under the “Methods” section, the probability of the occurrence in two proteins of just one heptapeptide is equal to ~ 20−7 (or 1 out of 1,280,000,000). Likewise, the probability of the occurrence in two proteins of just one hexapeptide is close to zero by being equal to ~ 20−6 (or 1 out of 64,000,000).
…A massive peptide commonality is present with humans and mice, i.e., organisms that undergo pathologic consequences following SARS-CoV-2 infection. Instead, no or a lowest number of common peptides are present in mammals that have no major pathologic sequelae once infected by SARS-CoV-2 [10,11,12]. Hence, the data appear to be an indisputable proof in favor of molecular mimicry as a potential mechanism that can contribute to or cause the SARS-CoV-2 associated diseases [8].
Self-similarity of foreign proteins can lead to autoimmune conditions. As the body attempts to halt a foreign protein intruder that looks like itself, it cannot distinguish the bad from the good. COVID infection and COVID mRNA vaccination can trigger autoimmune conditions. This is not surprising given the fact that the spike protein the vaccine creates all over your body looks remarkably similar (“highly improbable” mimicry) to your own proteins yet is marked by the immune system as an intruder. Antibodies form for the intruder’s patterns, but these can attack your own body since the intruder and body looks so darn alike.
Recent research fortunately shows that mRNA vaccination appears to avoid triggering the excessive auto-antibody development that COVID itself generates, and this latest evidence suggests the unique dynamics of COVID infection, not simply molecular mimicry, are to blame for auto-immunity. This is exceptionally good news, despite other papers showing vaccine-driven autoimmunity remains a concern.
And here’s something else—because of the intense mimicry, the COVID spike protein is likely one of the most biologically active agents that can enter our body. Many foreign proteins are relatively inert, as the body has no co-evolved mechanisms to interact with their patterns. But the spike protein and its many peptides can interact with myriad human protein cascades with unknown and unintentional effects, and we have growing knowledge of the breadth of toxicity and pathology induced by the spike protein on its own.
Researchers warned of “super antigen” characteristics of the spike protein in early 2020. Here we find damning evidence from April 2021 showing spike protein-induced damage:
In the new study, the researchers created a “pseudovirus” that was surrounded by SARS-CoV-2 classic crown of spike proteins, but did not contain any actual virus. Exposure to this pseudovirus resulted in damage to the lungs and arteries of an animal model—proving that the spike protein alone was enough to cause disease. Tissue samples showed inflammation in endothelial cells lining the pulmonary artery walls.
The Salk Institute led its announcement of the study, “a major new study shows that the virus spike proteins (which behave very differently than those safely encoded by vaccines).” The parenthetical is problematic and deceiving The evidence has been strengthened, but smart people understood early on the spike protein induced from vaccination in our cells was not some benign version that would be safely tethered by the smart design or sound mRNA platform kinetics. Those who did were delusional biologists, yet their message “won” for many months. In other words, the COVID “antivax conspiracy theory” was evidence-driven. Post-vaccine adverse events observed during the clinical trials (and in all their various manifestations in our post-vaccine world) can be explained by spike protein and mRNA platform dynamics.
For those who inject a bivalent booster, there are now two spike protein variations with intense self-similarity that the body must contend with (BA and Wuhan types). The fall 2023 booster just approved in the USA will give you the XBB type, yet is unlikely to trigger much variant-specific antibodies due to imprinting from your original (over)doses of Wuhan spike protein vaccines. This XBB boost was recently approved with zero clinical evidence or precedence—and please, please, please understand that this is not like annual flu shot adjustments.
We knew this COVID spike protein was highly risky stuff at the outset. Vaccinators, why did you select a super antigen with extreme (“mathematically improbably”) self-similarity that can trigger myriad bodily interactions and problems and you keep selecting it for variant boosters?
…you’ve injected the code for one of the most biologically active and toxic proteins known to humanity, likely of unnatural/hybrid origin, and the code is now distributed to cells throughout your body to instruct them to create the toxic protein?
Although many “disinformed repeaters” told us that the vaccine stays in your arm, it was actually designed encased in lipid nanoparticle technology that rapidly distributes everywhere in the body. The lipid nanoparticle and mRNA platform was observed in Pfizer’s own biodistribution study to rapidly travel to all major organs with more-than-negligible concentrations in the ovaries, adrenal glands, bone marrow, and even showing up in the brain, spinal fluid, and bone.
We were also told the spike protein resulting from vaccination will somehow be safer than the wild type, unable to bind/interact with our native cells, and will be safely “tethered” to the cells that produce it—nothing like the scary, pathological spike protein you find in COVID natural infection. One can find numerous factchecks and articles that advance these disinformation talking points to this day with zero valid evidence, including the prior Salk Institute release on spike protein toxicity. This seems to be a prevalent bias of modern USA, since many “believe” vaccines can do no harm.
Ponder for a moment what happens to the human cell that has so nicely generated and “tethered” a bunch of COVID spike proteins? Our body’s immune system will typically bind and/or attack it, cleaning it up, but the spike protein and fragments (including its S1 and S2 subunits and smaller, which also pose troubling biological activity) can certainly end up spread about (everyone seems to have conveniently forgotten or somehow didn’t think basic human biology like cellular necrosis would apply to this duplicitous technology), as shown in multiple studies and for many days following vaccination:
…there is likely to be an extensive range of expected interactions between free-floating S protein/subunits/peptide fragments and ACE2 circulating in the blood (or lymph), or ACE2 expressed in cells from various tissues/organs (Figure 2) [14., 15., 16.].
Significant free spike was found in a recent myocarditis study by the American Heart Association (AHA), and in exosomes persisting for no less than 4 months, which, at best, may serve as unhelpful decoys for antibodies, and at worse cause more havoc as they spread and contact new cells (you can vaccinate mice with these exosomes alone, per the study). From the AHA’s January 2023 study:
A notable finding was that markedly elevated levels of full-length spike protein (33.9±22.4 pg/mL), unbound by antibodies, were detected in the plasma of individuals with postvaccine myocarditis…
Fortunately, the study authors did not find free spike protein in 45 vaccinated “control” recipients who did not succumb to myocarditis, but this could simply suggest complete binding of the spike with vaccine-generated antibodies at the time of testing, inconsistency across vaccine product, or other patient factors. What happens to these patients if additional spike proteins are generated from persistent vaccine mRNA, subsequent shots and “immunological tolerance” (explored next), and repeated reinfection, for example?
It is clear the vaccine-induced spike protein and smaller fragments are showing up free floating in the body (unbound by antibodies), comparable in some studies to severe COVID, and this has been associated with its myriad toxic side effects.
For what it’s worth in terms of explaining pathologies and also contrary to most “fact checks, the “prefusion-stabilized” form of the spike protein that the vaccine is supposed to encode can still bind and interact with cellular ACE2 receptors in its prefusion state via its receptor-binding domain (RBD). This study finds that the prefusion-stabilized spike protein from the Novavax vaccine (essentially the same “prefusion-stabilized” protein as Pfizer and Moderna but via a non-mRNA platform) “clearly shows binding to ACE2, indicating that the RBD is dynamic and the receptor binding site accessible,” this study finds “the binding of expressed and purified [Pfizer BNT162b2-generated spike protein] S(P2) to ACE2…,” and this one found the same binding with pre-fusion Astra Zeneca spike protein, along with an important qualification:
While this observation that the majority of cells infected with ChAdOx1 nCoV-19 present native-like spikes on the cell surface (Figure1B), it is interesting to note that a population may shed the S1 subunit.
The spike proteins many assumed would be safely tethered to the surface of a cell shed the harmful S1 subunit.
The spike protein, its S1 and S2 subunits, and smaller fragments are toxic to heart cells, neurodegenerative, amyloidogenic, and the improbably-high molecular mimicry with human proteins can trigger all sorts of biological pathways.
The spike protein mRNA is distributed shortly following injection to all our major organs and systems, where it transfects our cells and promptly generates COVID spike proteins. There is no evidence to suggest the modified COVID spike protein from vaccination is somehow more safe, benign, or inert, than the spike protein found on the virus. In fact, the evidence suggests COVID spike protein toxicity, harm, and biological activity is similar (and in many cases, potentially worse) from vaccination as compared to infection. Consider seriously the implications of this post-vaccine case report—everything went haywire.
Validating evidence and concerns expressed as early as 2021 of vaccine-induced Stevens-Johnson syndrome/toxic epidermal necrolysis (SJS/TEN), a 2023-published study on the rare skin disorder, SJS/TEN, was just released in which researchers found a 7-fold increase in the disorder since the beginning of the pandemic, including:
In the first six months of 2022 however, we managed fourteen cases. Five of these cases had COVID in the preceding month. Three of the fourteen had a COVID vaccine in the preceding month. All fourteen cases received a COVID vaccine.
None of the cases were among the unvaccinated. This complements so many other pieces of compelling evidence that depict the vaccine wrecking things internally and making COVID itself worse. Given the rarity of the condition and limited number of unvaccinated people in the study population, the authors of the 2023 publication acknowledge no casual inferences can be made, and they offer “virus-induced” and “vaccine-induced” explanations. Other available evidence describes in detail the mechanisms of vaccine damage that could account for these observations. I call it simply, “spike protein overdose.”
About 1.5% of the administered dose is measured in the small and large intestines 48 hours after vaccination, based on Pfizer’s biodistribution study. The gut also includes a prevalence of ACE2 receptors. Evidence of significant and persistent damage to the microbiome after vaccination is concerning, as is the cellular damage. “Mysterious” gut issues have an easy explanation these days.
Pfizer and the FDA attempted to cover up their biodistribution study of LNP-mRNA platform (and then they tried to delay ongoing FOIA’s), which the Japanese were the first to successfully obtain and release in redacted form. TrialSiteNews looked into this in great detail in their coverage. Others, through ignorance or deception, attempted to diminish the early studies on vaccine biodistribution and related propensity for vaccine-induced spike protein interaction, damage, and pathology, in spite of the most basic evidence of danger and harm. Vaccinators, why do you continue to blame anything but the vaccine for the myriad post-vaccine pathologies we understand can be triggered by the spike protein it generates across our cells?
…the code you’ve injected and is now distributed throughout your body is based on nature (mRNA) but has been genetically modified to ensure it does not disintegrate too quickly, and no one knows (or is telling) how long it persists in the body or how much spike protein it creates?
The mRNA has been stabilized with a 1-methylpseudouridine substitution (m1Ψ mRNA). This was done to ensure the body generates enough COVID spike proteins following vaccination before enzymatic processes breakdown the mRNA. We still do not know how long it will take for the stabilized m1Ψ mRNA to be fully degraded by natural bodily processes (which degrades “natural” mRNAs swiftly) and halt its production of spike proteins.
We know that the stabilized m1Ψ mRNA and spike proteins are persisting for at least 15 days in this report, and for at least 28 days in this one. Whether due to being encased in lipid nanoparticle (LNP) and/or due to the mRNA “stabilization trick”, these authors speculate for the mRNA vaccines:
…this allows prolonged spike protein production giving an advantage for a continuous immune response in some persons.
The mRNA vaccines will allow for “prolonged spike production.” Which will result in a “prolonged” immune response. In other words, prolonged inflammation. Is this advantageous?! And is informed consent a thing at all anymore?
The body may be pumping out background levels of COVID spike protein indefinitely for all we know. (And remember, antibody titers are not a valid metric for success!)
We know that the spike protein is toxic on its own, and there is evidence of excessive immune response following vaccination, suggesting excessive antigen presentation. From the recent preprint of an independent genetic researcher (whose work includes collaboration on MIT’s human genome project), Kevin McKernan, we find one of the most obvious yet underappreciated logic chains of our modern COVID era:
Finally, the pharmacokinetics of injection are different than infection. 30ug- 100ug per injection (90ug-300ug for those boosted) of Spike mRNA equates to 13 Trillion to 40 Trillion mRNA molecules injected in a few seconds with each injection. The pharmacokinetics of this bolus injection differs from that of viral replication that occurs over the course of a few days. If each of these mRNAs can produce 10-100 spike proteins and you have 30-40 Trillion cells, there may be a far greater systemic quantity and a much longer duration of spike protein exposure through the vaccination route than natural infection. Boosters given more frequently than a year will lead to total body accumulation of spike protein and further heighten the risk of disease in organs such as the brain, heart, bone marrow, and immune cells and tissues. This false equivalency may lead to an under appreciation of the symptomatology of vaccine based adverse events.
This is backed up by measured post-vaccine spike protein and S1 subunit concentrations in this peer-reviewed paper (“post-vaccine study”) achieving levels after the first shot comparable to (and for longer than) severe cases of natural COVID infection (“natural infection study”) before diminishing rapidly through narrowly-focused and extremely-elevated antibody response. Antibodies bound up the circulating free spike in most patients after the second shot. What of the 3rd, 4th, 5th, and 6th shots, and so on…?
Preprints and data of the “post-vaccine study” was shared with the world on May 20, 2021, when most “low-risk adults” were lining up for the first jab:
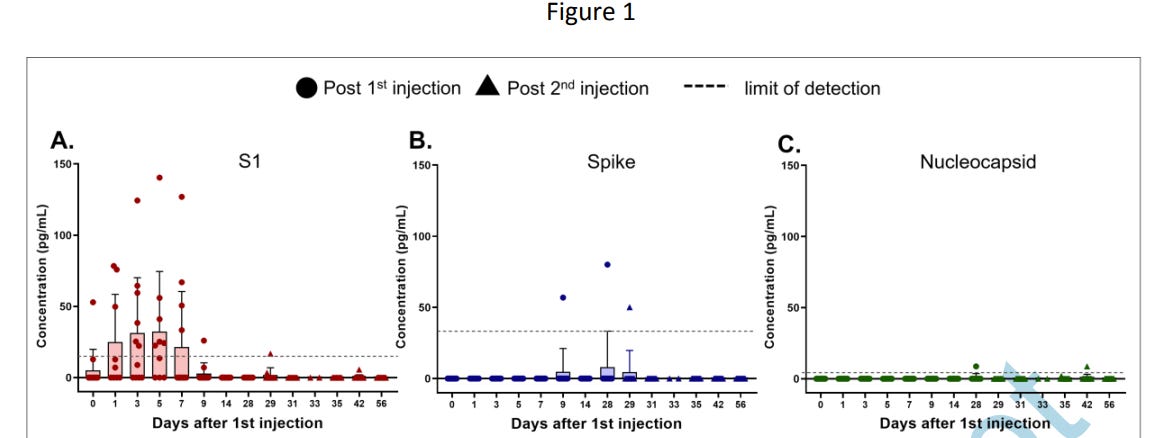
They report freely circulating S1 subunit following the first vaccine dose in 11 of 13 studied patients. “The mean S1 peak level was 68 pg/mL ± 21 pg/mL” following vaccination.
Comparing S1 levels in patients with natural infection (unvaccinated), the “natural infection study” authors, including David Walt from the post-vaccine study, found 23 of 64 COVID positive patients had zero detectable free S1 subunit during infection. Twenty-three patients had “low concentrations of S1 (6–50 pg/mL)” and the remaining 18 patients had “high concentrations of S1 (>50 pg/mL).” Each group corresponded to increasing rates of COVID severity, with most of the “high concentration” patients going to the hospital with severe COVID.
Ok, post-vaccine, 11 of 13 patients had mean S1 peak level of 68 pg/ml ± 21 pg/mL. And post-infection, patients corresponding with greater COVID severity were categorized with “high concentrations of S1” greater than >50 pg/mL, which was found in fewer than a third of infected patients. All other infected patients had considerably lower levels or S1 (with more than a third having completely undetectable free S1) than the post-vaccine average.
The S1 concentrations found in plasma post-vaccine readily exceeded the “high” levels measured following natural infection (even on average!), and for many days on end.
In prominent fact checks at the time (during the first wave of “low-risk adult” jabbing) co-author to both studies, Walt, discounts and diminishes the post-vaccine spike and S1 concentrations, calling the post-vaccine S1 subunit measurements a “very low concentration,” with no valid argument using the data they reported and that I just shared with you.
We still don’t have a great handle on the actual dosage of mRNA in each shot, how many spike proteins that will generate, and when the mRNA is fully degraded given it’s synthetic m1Ψ stabilization. But we knew right away that the vaccine was generating its target antigen, the COVID spike protein, in extreme quantity, exceeding on average even the most severe cases of natural COVID infection. Dear Vaccinators, why are you dosing us with so much antigen, and when does the vaccine “stop”?
…you may have taken a heroic dose of COVID spike protein through repeated vaccination and your antibodies start converting to “tolerant types”?
Conversion of inflammatory IgG(1-3) antibodies to non-inflammatory IgG4 types is showing up among the vaccinated after two doses, as if we are overdosing on the antigen (spike protein) and creating an “allergen” type of response to the spike protein (similar to a bee sting response). From the authors:
We detected spike-specific IgG4 antibodies in about half of the serum samples collected 5 to 7 months after the second immunization, all of which did not show any IgG4 at earlier time points. For all other IgG subclasses, a decline was seen in the same period. Moreover, after the third immunization, IgG4 levels sharply increased and became detectable in almost all vaccinees.
IgG4 class switching has been found also in cases of severe COVID, but not so much in mild cases (see this study from Brazil, for example). We have no idea the full ramifications, but this could lead to immune tolerance toward COVID and possibly minor but longer/indefinite infections that spiral variant evolution alongside repeated infections and diminished immune function across the board. “Smoldering,” ongoing infection and systemic inflammation may be our new normal. Whether from IgG4 class-switching, immune imprinting, antibody-dependent enhancement, immune exhaustion, and/or other factors, the vaccinated have more COVID reinfections for every successive boost.
IgG4 didn’t work out so well in prior HIV studies and it was correlated with more severe natural COVID infection outcomes (possibly generating because of the outcome, however). IgG4-related disease is also a possibility, which can lead to gradual and ongoing organ damage.
Even the most “serene” opinions on vaccine-induced IgG4 that I’ve seen—this one—comes out with:
on the basis of the results of the studies discussed here and other theoretical considerations, future clinical studies need to evaluate the effectiveness of temporal spreading out of mRNA vaccine boosts—possibly no more than once a year. Other approaches worth investigating would be the use of smaller quantities of mRNA for booster doses and, separately, the use of mRNA vaccines for priming only, with heterologous boosts with adjuvant-free recombinant spike proteins because, theoretically, adjuvants are most relevant during priming and may not be necessary for boosting.
Boosters “no more than once a year,” which I believe is wholly too generous given the risk profile, especially assuming you will have some natural infections in the interim—but that’s the serene take. And don’t hold your breath on those clinical studies—FDA just authorized the fall 2023 boost based on a hunch.
Now, a May 2023 peer-reviewed article in Vaccines states:
emerging evidence suggests that the reported increase in IgG4 levels detected after repeated vaccination with the mRNA vaccines may not be a protective mechanism; rather, it constitutes an immune tolerance mechanism to the spike protein that could promote unopposed SARS-CoV2 infection and replication by suppressing natural antiviral responses. Increased IgG4 synthesis due to repeated mRNA vaccination with high antigen concentrations may also cause autoimmune diseases, and promote cancer growth and autoimmune myocarditis in susceptible individuals.
Yikes. And although natural minor reinfection among vaccinated folks can trigger additional IgG4 class-switching, as far as I’m aware, there is no evidence that the unvaccinated experience any significant IgG4 class-switching following repeated natural minor infections.
Given the scary pathologies of COVID, perhaps developing “tolerance” to COVID is an effective strategy for buying a few more years of life for those “at-risk” (certainly not the general population), but thus far it seems to be backfiring. Perhaps this was the whole point of these mRNA technologies, and nobody wants to talk about it?
This class switching seems to be an artifact of extremely high dosing of antigen (COVID spike protein) from the vaccines, and/or associated with an inherent immune response to the lipid nanoparticles and/or synthetic mRNA.
The potential ramifications for life-long immune function, homeostasis, and susceptibility to future COVID infection from IgG4 antibody class-switching is significant. Vaccinators, are you still bullish on IgG4 or should we maybe start talking about this with the public?
…you instruct your stem and germ cells to create COVID spike proteins, which should then be targeted for attack and immune system activation (and some are probably “privileged” cells)?
The public now knows the LNP-encased mRNA distributes to every major organ and bodily system based on Pfizer’s studies (including the biodistribution study originally held back from public release), including bone, bone marrow, ovaries, the brain, spinal cord, everywhere, where it transfects and inflames your native cells. Voluntary meningitis for all. To be clear, natural infection spreads virus, but infection of bone marrow and spinal fluid in the first hour? Probably not.
There is a fundamental flaw (well, several) in this platform that needs addressing: if a partial antigen (in this case, the COVID spike protein, just a piece of the virus) is presented to the immune system by native cells via mRNA transfection, how does the immune system deal with “chimeric” partial antigen/self-cell? Does it pursue a novel pathway? Does it create a valid instruction/pattern recognition to attack the spike protein when challenged by COVID-19, or will it also include some of the self-cell definition and novel auto-immunity? Is the pattern definition sufficiently broad to address future viral variants? How is this distinct from the natural/viral infection of many cells types, which may pose similar challenge?
Evidence suggests that the vaccine does indeed introduce novel and likely damaging immunological dynamics (IgG4 case in point), but auto-antibody development may be diminished from vaccination, especially relative to COVID itself. Evidence appears conclusive that extremely narrow antigen pattern mapping and imprinting from excessive Wuhan spike exposure leads (primary series) leads to diminished variant-specific antibodies and enhanced susceptibility to future COVID variants. An unending pandemic.
It sure does seem the vaccinators have an underqualified understanding of the Major Histocompatibility Complex (MHC) molecules and the process of MHC presenting “patterns” of foreign antigens to T cells for immune definition.
Now, since we know through the biodistribution studies that the vaccine will quickly transfect all cell types, including stem and germ cells, particular considerations need to be made. Stem cells and their niches can maintain various “immune privileges,” where the immune system ignores or responds to stem cells differently than other cells given their unique function.
What happens when stem cells start pumping out COVID spike proteins after they are immediately transfected by the mRNA vaccine? Do the spike-laced stem cells wreak havoc in various immune-privileged states, as the immune system is unable to constrain them? Or does the spike protein suddenly attract the immune system to destroy the stem cell, overriding any privilege with novel immunology? What LNP-mRNA, spike protein, and immune responses are mediated that could compromise stem cell viability (count and function) in marrow and other sensitive sites?
Our body works hard to prevent natural viral infection of our bone marrow, yet it is hit by spike protein mRNA and transfected within several hours of injection thanks to the LNP coating.
As for other unique cell types, like germ cells, we see a 22% decline in total motile sperm counts following vaccination for several months, as reported in this Andrology article. Old news, but young men need to know this, as their fertility is diminished for a quarter. Fortunately, sperm are renewable!
How many of the lifetime-fixed number of eggs are compromised in women, if any? The sex organs seem to be a hot spot for vaccine biodistribution per Pfizer’s study, and although less than 1% of the studied injection platform was found in ovaries at time points between 0 and 48 hours, we have no idea what’s happening to oocytes following repeated and ongoing mRNA transfection. A small study of 128 women (26 vaccinated) found a 2.2% reduction in sustained implantation rate of embryos in IVF in the vaccinated (those who had taken the Moderna and Pfizer primary series) as compared to those who were unvaccinated, concluding in the most positive way that the vaccine does not “impair infertility.” Yet they documented a negative vaccine effect on fertility (63.7% vs 61.5%, p value 0.1).
(Let’s remember for a moment that the “95% vaccine efficacy” we were sold from original clinical trials equated to an 0.84% absolute reduction of COVID infection risk as measured through number of “positive PCR tests.” The point being that a 2.2% absolute decline in an average medical outcome is really big. A larger sample size is a must to validate one way or another.)
To be clear about the study above, COVID infection was worst of all for embryo implantation rates (54.6%), yet there is no evidence presented that vaccination would help with this. Other research suggests we will probably find that COVID infection plus vaccination is worst of all, and since vaccination doesn’t stop infections, well.
And what’s the additive and cumulative effect of additional boosters? Especially as egg count and quality trends down rapidly in your later 30s, any introduced damage to oocytes and implantation rates can make or break fertility—a much larger study, evaluated by age, should be demanded by…people. Folks are clearly still having kids, but this matters greatly to mothers-to-be. It’s only maybe safe for your ovaries, on average, maybe. Global fertility rates will be affected post-vaccination / post-COVID.
Note the complete absence of knowledge on risks to fertility from these injections, especially repeated and cumulative effects, administered to pre-pubescent and adolescent children.
You see, the early assumption was that this would be a “once and done” vaccination. People contextualized all understanding of safety and efficacy around this idea. The cumulative effects of repeated dosing are taboo for many, but like the IgG4 class-switching effect, ongoing injections are diminishing us and evidence suggests the damage will be broad.
The potential implications for lifelong health are tremendous, but the science has not been pursued nor required by our regulators. Vaccinators, will you explain to us why you think it is safe to repeatedly transfect germ and stem cells with synthetically stabilized spike protein mRNA, even if in small dosage?
…the spike protein freely circulating your body is now inhibiting tumor suppression pathways that have been critical for keeping benign tumors, existing cancers, and homeostasis in check?
The spike protein and its subunits bind to tumor suppressor P53 and breast cancer gene BRCA, which is plausibly associated with an increasing incidence of aggressive, metastasizing, and expediently-mortal cancers. This article explores the associations of the spike proteins molecular mimicry with tumor suppressor peptides, suggestive of an elevated cancer risk following any exposure to the COVID spike protein, including from vaccination. The authors state:
This article described a vast peptide overlap between SARS-CoV-2 spike gp and tumor-suppressor proteins, and supports autoimmune cross-reactivity as a potential mechanism underlying prospective cancer insurgence following exposure to SARS-CoV-2.
(And I have already presented evidence for why we should not assume the spike protein from vaccination is somehow more safe and benign in spite what one might find in poorly-researched fact checks; it is likely worse as it embeds throughout your body and many cells types rapidly via LNP transport, whereas infection can be inhibited by your immune system to stall its spread to organs, marrow, spinal fluid, and so on. Evidence shows serum spike protein/subunit levels are extremely high following vaccination. Reinforcing the dynamic is the fact that one is more prone to repeated natural infection and “spike protein exposure” with every additional boost.)
I contend that this fall 2022 story of a post-vaccination cancer diagnosis in The Atlantic is not a unique story, and personally I know of several who have experienced unusual development of new or resurgence of prior cancers that the body was seemingly keeping in check prior to vaccination. There are many plausible paths to triggering cancers from vaccine, including overall immune exhaustion and mRNA-induced antigen production by stem cells. But one thing is clear, we have now entered a new era of turbo cancers, exacerbated by all our various environmental issues and genetic predispositions. Vaccinators, why didn’t you bother to look at toxicity and cancer risk from these novel and experimental products, especially when you knew they would transfect every cell type?
…if pregnant, you end up with three times fewer hematopoietic progenitor stem cells in the umbilical cord blood of your developing fetus/baby, with the most loss occurring when vaccinated earlier in gestation (“indicating that factors causing these damages are maintained over the gestation period”)?
Hematopoietic progenitor stem cells differentiate to form your platelets and white and red blood cells and are critical throughout life. In a 2022 publication, natural COVID infection was found to cause worrisome destruction of these vital cells in a developing fetus’ cord blood, but the researchers found that COVID vaccination during pregnancy led to far worse outcomes (1.7-fold from infection vs. 3-fold reductions from vaccination). This occurred via induction of apoptosis (programmed cell death) of hematopoietic progenitor stem cells (HSPC). The authors of this finding report “unprecedented concerns on the future of HSPC-based therapies” (e.g., stem cell transplants for adults), but since they do not focus on pediatric outcomes, there is no speculation about impacts to the developing fetus and infant health. One can find plenty out there on the importance of these critical stem cells in life-long immunity, such as “Fetal Hematopoietic Stem Cells Are the Canaries in the Coal Mine That Portend Later Life Immune Deficiency.”
Now, in this study, authors found:
that maternal and cord blood IgG antibody levels were higher after COVID-19 vaccination compared with after SARS-CoV-2 infection, with slightly lower placental transfer ratios after vaccination than after infection.
The average maternal IgG antibody concentration among 169 vaccine recipients was more than 10 times higher than levels found among 408 persons with natural infection. And:
Similarly, the geometric mean cord blood IgG concentration of neonates born to vaccine recipients was significantly higher compared with the geometric mean cord blood IgG concentration of the neonates born to persons with infection (Table 2).
That the vaccine induces 10 times the amount of IgG antibodies in umbilical cord blood as compared to natural infection is telling. Antibodies are not what your body craves—they are more nuanced and can often be detrimental. The antibody levels were higher from Moderna injections than Pfizer, which is obvious since Moderna contains a higher dosage of mRNA. Overdose on spike protein?
The evidence from these two reports demonstrating HPSC destruction alongside spike protein antibody concentration in cord blood following vaccination that far exceeds natural infection is a serious safety signal. Serious.
Is this a case of vaccine-induced auto-antibody development unique to pregnancy? Or is there free/partially bound COVID spike protein causing damage? Does this relate to excessive antibody response and conversion to immuno-tolerant IgG4?
As a reminder, Pfizer failed to complete its promised trial in 4,000 pregnant woman with no publications made, stalling out at 349 enrolled participants, which in any case is far too small (remember, the original Pfizer and Moderna clinical trials found on average 1 in 800 vaccine injections led to severe adverse events—hospitalization, disability, and/or death—so even this elevated incidence of adverse events would be missed with a study of only 349 pregnant women). There may be a forthcoming report from the trial that started in 2021 (result appear to have been provided in July 2023 but nothing has been posted), but of course, they didn’t get to their intended 4,000 patients to study. This study intended to look at some things beyond the “standard” 60 days after vaccination, such as downstream fetal and infant outcomes within the first year of life.
We already messed up by allowing mRNA injections during pregnancy with no legitimate safety data (hopefully for the most part on principle). We most certainly cannot continue subjecting every newborn of this generation to such uncertain fate, whether through vaccination during pregnancy or early infancy, without some actual long-term, placebo-controlled safety testing!
That OBs recommend this stuff—we are witnessing some significant “head-in-sand” mind warping and lack of curiosity given the prolific evidence and potential for harm (and never safety) to both mother and infant.
Vaccinators, will you let us know why you are comfortable with the post-vaccine slaughter of hematopoietic progenitor stem cells in fetal cord blood during pregnancy, at rates far exceeding natural infection, since you do not appear committed to further clinical study on pregnancy or fetal and infant outcomes?
…the mRNA concoction you’ve injected is contaminated with its plasmid (dsDNA) precursors, mistranslated mRNA segments, and broken fragments?
There is no consistent quality control testing of the finished mRNA vials, only estimates of how much is fully encoded in finished vaccine vials with limited oversight. Some are finding concerning contaminants, including incorrect mRNA segments and smaller fragments. Although researchers fortunately have found that the mRNA fragments in Pfizer vials did not translate unexpected proteins, lots of odd stuff can arise in the body from random mRNA sequences floating around.
A recently published letter to the European Journal of Clinical Investigation found statistically improbable inconsistency of reported, suspected adverse events across vaccine lots that “suggest the existence of a batch-dependent safety signal for the BNT162b2 vaccine.” A small number of batches are contributing most of the suspected adverse events, which implies significant inconsistency of the finished product that is showing up across batches.
Notably, research has also provided evidence of DNA plasmids as contaminants, including the SV40 promoter, which are used to produce the mRNA and are supposed to be purified away. (See primary sources here and here for recent CLIA lab confirmation of presence, which has now been replicated independently from different vials and parts of the world).
In their latest summary prepared for FDA presentation, the researchers state:
Using multiple analytical methods we determined the dsDNA contamination was 18-70 fold over the 330ng/mg DNA/RNA guideline set by the EMA. It is also over the 10ng/dose guideline by the FDA.
Since the plasmid DNA includes “production waste” gene segments from the precursor strains of E. coli (which have been made resistant to the antibiotics kanamycin and vancomycin), these may infect bacteria in our system. This can result in some odd behavior, such as innate bacteria replicating and serving as a “bactofection source” for plasmid infection of our mammalian cells.
Dynamics that result from injecting the remnant SV40 promoter insertion are poorly understood, with metastatic cancer a primary concern:
SV40 virus is a controversial sequence as it contaminated the polio vaccines and is still debated to this day if it caused 100 million cancers. While the vaccine does not contain the full virus sequence, 2-20% of the population is believed to be SV40 infected in part due to the polio vaccination program. It is not known what will happen if we inject SV40 infected patients with large quantities of SV40 promoters, enhancers or origins of replication.
The research also suggests reconsideration of the potential integration of the COVID spike protein mRNA into the human genome, including this recent summary:
These nuclear integration risks are not hypothetical. They are the reason the FDA has these limits as described by Keith Pedens work. To further emphasize this point Strayer et al demonstrate even fragments of plasmid vectors can integrate into the genome with SV40 containing plasmids. Gonin and Gailard discuss the biodistribution risks of various gene therapy vectors. Banoun et al. describes why these mRNA vaccines qualify as gene therapy.
“These SV40 promoters contain a strong nuclear localization signal known as the 72bp SV40 enhancer,” which is known to enter the nucleus. And, what do we then make of the plausible transfection of germ cells by dsDNA-contaminated mRNA? Have we altered the genome with duplicitous Pfizer potion? Seriously asking.
To wrap this up simply:
These contaminants are over the limit. Multiple independent scientists are reproducing these results. The injection of dsDNA containing controversial DNA sequences known to integrate into the genome was not properly disclosed to regulators nor patients in the informed consent process.
A non-biased, nuanced summary of the situation for the lay reader is available here.
Evidence regarding Pfizer product inconsistencies points toward two distinct manufacturing processes that were used, and that a majority of adverse events may be showing up in a “never-trialed” second process, which was only tested on 250 patients (“Process 2”). And, as usual, regulators have not helped scientists investigate, and supposed experts diminish without investigation. Moderna deserves its own, separate scrutiny, but investigations to date have not revealed dsDNA contamination in Moderna vials.
Australians are suing. Hopefully other suits will follow. Special COVID-era liability protections in the US will make suits complex or impossible, but cases are being built around failed compliance and regulatory accountability in the “military countermeasures” operation that is this pandemic. People cannot remain immune from liability for developing, distributing, marketing, and injecting contaminated and dangerous products, the failed countermeasures we label as COVID vaccines, to a susceptible population. The idea that we need liability protections to enable “vaccine innovation” like this has always been flawed—why worry about safety when you can run the corrupted clinical trial traps and end up with no liability? Note that taxpayers are on the hook for what meager payments we do provide to victims of vaccine damage.
Dearest Vaccinators, as the rogue citizenry is opening vials (illegally, I might add, because of reasons) and validating dsDNA contamination results across the globe, will you maybe look at a few of the vials yourself with an independent monitor and get back to us? And then remove the liability protections for vaccine manufacturers and COVID era countermeasures, maybe?
Ask the Questions
As of May 2023, only 17% of those eligible in the US have taken a bivalent booster (originally offered fall 2022). This is in sharp contrast to original waves of mRNA uptake, which I contend was catalyzed by:
Imperfect information on both risk and benefit during a period of intentionally seeded fear and isolation (trauma),
Deception and fraud in primary scientific investigations and communications that catalyzed a broader network of disinformed “repeaters,” and
For many, forced exposure through employer and federal mandates, severe restrictions like prohibited access to stores or restaurants for the unvaccinated, and other radical peer pressures.
The people of the USA, where mRNA vaccines remain widely accessible and recommended for ages as low as 6 months (none of our peers continue to allow for this), seem to be increasingly aware of these evident truths and outstanding questions of concern. Yet big media communications and fact checks remain biased in favor of vaccine uptake and repeated boosters as frequently as every 6 months. Hold right up. Ask the questions. Look at the evidence.
It is hard to underestimate the implications of what we see unfolding to this very day—the social implications, like a growing disinformation and censorship complex that many tolerate, even embrace, as well as the medical implications given what we know today and can foresee. It is vital that we begin to acknowledge our past mistakes, ongoing atmosphere of deception and fraud, and hold folks accountable with new evidence gained. We also must work to heal our divides and our damaged health.
Corporate pharma leaders know and/or don’t care about the many critical concerns and questions about the safety profiles of the latest experimental mRNA therapies that express the COVID-19 spike protein. They maintain the “safe and effective” charade and pursuit of profit. The regulators are asleep, brainwashed, or brainwashing. And, in any case, they hold back critical data. The big scientific journals are beholden to conflicted boards of regulators and drug makers (as a prior editor of BMJ warns us), and leaders in academia corrupt science alongside naïve proponents. Doctors are threatened professionally (the threats began early on and continue to this day) and censored for exposing their evidence-based viewpoints.
And the rest of us are gaslit or waking up to the tendrils of mis- and disinformation that enabled this pandemic, COVID-19, and the slop “vaccines” that fail to meet any standards for safety and efficacy. FDA can’t even figure out what to analyze for updated boosters given the absence of any objective efficacy standards or performance goals, since the rapid waning of the primary series and boosters fails to meet their own stated efficacy standard. Efficacy for “how long”?
estimated vaccine effectiveness against both laboratory-confirmed Omicron infection and symptomatic disease was lower than 20% at 6 months from the administration of the primary vaccination cycle and less than 30% at 9 months from the administration of a booster dose
This looks like a (genetic) therapy, not a vaccine. If our standard has evolved to reducing severe outcomes and death, a better all-outcomes risk-benefit framework for medical therapy is needed before FDA advisors continue winging it with their booster recommendations. Unfortunately, I suspect they know what they will find (the evidence is out there, as I have shared) and will avoid looking too hard. The fall 2023 booster approval was exemplary.
Our deeply-rooted, cultural bias toward vaccines being “safe and effective” to the point that we do not question and study even the most basic assumptions makes it easy to be complicit in the perpetual lies, obfuscation, and poor decision-making.
It is harder and harder to not see what is going on, however. Most have likely personally witnessed the evidence of harm at this point, assuming the appropriate dots are connected with the abundant (but censored and silenced) clinical research and evidence. The alarm is hence getting louder and louder. And our intuition and collective behavior becomes more cautious—“it’s not worth it.”
The research has been highly suggestive for some time of a “story” that diverges substantially from mainstream accounts, and a growing populace is reconsidering past evidence they may have missed or glossed over. Here is a quote from Science in January 2022:
Cheng has heard from dozens of people who describe chronic postvaccine problems, and she finds the overlap between their symptoms and those of Long Covid compelling. Now, she wants to move deliberately and scientifically in a search for answers. “We’ve got to retain rigor,” she says. “There’s just this complete dearth of data.”
This article hints at the inability to “speak openly” about such topics. And, as we have seen in every vaccine-related article scrutinizing and critiquing its effects and propensity for harm (here’s another good example), the authors include the oft-repeated boilerplate, “the risk of complications from SARS-CoV-2 infection far outweighs that of any vaccine side effect,” with no mention of risk-benefit (i.e., is risk of Long Vax worth benefit, if any, gained?), and which is out of scope for the research when used. I call it the disinformation “safety blanket.” So even if the vaccine is causing long COVID (it is, plus more reinfections and a compromised immune system…), the consistent spin is that it won’t cause it as frequently as COVID infection itself and is worth it, based on zero research of net benefit or harm cited or presented.
Here we arrive at Science in July 2023 acknowledging “long vax” is taking people down, the vaccine causes POTS, and so on:
“You see one or two patients and you wonder if it’s a coincidence,” says Anne Louise Oaklander, a neurologist and researcher at Harvard Medical School. “But by the time you’ve seen 10, 20,” she continues, trailing off. “Where there’s smoke, there’s fire.”
But don’t worry, the article argues, these situations are still pretty rare, as it begins trailing off…
Remember, the few risk-benefit analyses that do exist continue to show more risk than benefit from mRNA injection and transfection and, well—have I done anything here to persuade you that we are well over our skis on the evidence for the substantial and long-term risks?
Vaccine-induced “long vax” and all the other harms the vaccine can induce are easy to witness among personal networks (small uncontrolled samples). Among my own, it’s intense, and for everyone I ask, there are plenty of case studies to hear about. Although many are still prone to blame other factors or COVID itself given the thick fog of disinformation and disbelief it could be “this bad,” there is a body of evidence showing that the vaccine is uniquely capable of triggering extremely aggressive blood cancers, tumors, and unusual metastasis, layered viral and bacterial infections, latent infections, demyelinating diseases/MS, tooth loss, insulin resistance, gut disbalances, anxiety and brain fog, neuropathy, Bell’s palsy, inflamed and enlarged hearts, “arrhythmias,” afib, pacemakers, high blood pressure, micro and major clots, strokes, sudden adult deaths, autoimmune disease, skin rashes/necrosis, more COVID re-infections, and so on. It’s a biological multi-tool, along with COVID itself, that is exacerbating human disease.
The evidence of (not rare) systemic harm is in front of everyone’s eyes, and scientific studies help corroborate and explain it. I have shared many here. The obvious contrast between what many “heard” and what is actually occurring is too hard to ignore, and this is leading to growing mistrust and skepticism about far-reaching topics. As people lift the veil, this has become a black swan in politics, medicine, and life in general.
Beyond the specific risks and harms of COVID spike protein mRNA transfection, this January 2023 paper explores broad concerns about impacts to our entire micro RNA bodily machinery following the mRNA shots. This April 2023 publication explores potential for harm from the LNP-mRNA platform itself, in addition to the potential for spike-protein-induced / COVID mRNA harm, suggesting a safe mRNA product may be possible, but certainly not in this case. There is a reason the LNP-mRNA cocktails previously failed for cancer and other uses—COVID saved Moderna and made BioNTech. Yet, what you are now beginning to hear and see from our corporate leaders is that this is only the beginning, and the vaccinator profit-seekers will iterate new mRNA injections for viruses du jour with little regard for the science of safety and efficacy.
For those willing to question their faith in the safety and efficacy of mRNA technology, there is abundant scientific evidence to debunk the dogma.
Epilogue: The Biodistribution Study
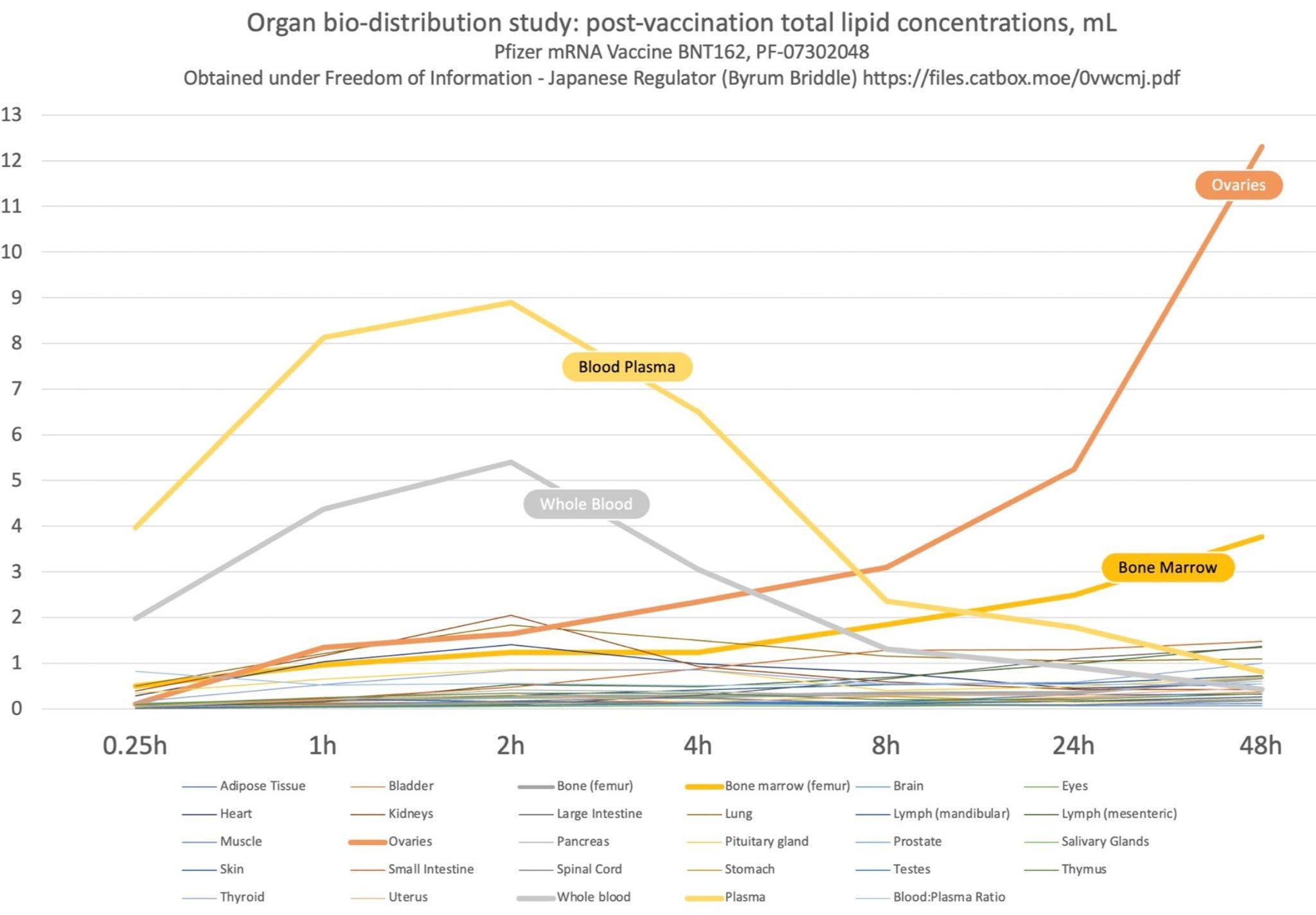
Pfizer’s biodistribution study evaluated the distribution of the lipid nanoparticle-mRNA platform following injection (it did not use the final spike protein mRNA). A Japanese government release came out in ~June 2021, and later it was released in English by US FOIA—this document was intended to remain sealed for decades. Although plenty out there have dismissed its findings as benign, I remain deeply skeptical of the supposed safety profile upon review of this evidence.
By using a radioactive marker, the study found the “mean lipid concentration” in ovaries at 48hrs following injection was 3% of the mean concentration measured at the injection site when it peaked at 1hr (12.3 micrograms/g in ovaries vs. 394 when peaked at the injection site). The data stops at 48hrs and the lipid concentration in ovaries is still rising.
Lipid concentration in bone marrow is also still rising at the end of the study at 48 hours, when it represents about 1% of the mean concentration measured at the injection site when it peaked at 1hr (3.77 in marrow vs. 394 at injection site).
These may be degraded lipids, and not representative of the presence of mRNA or spike protein, but it’s the best data we have from Pfizer to go by.
The study shares the percent of total administered dose arriving in organs, as well, which are small but not brush-aside-able in my humble opinion, with ovaries seeing 0.1% of the total administered dose at 48 hours (not a cumulative measurement). What also caught my attention is that between 24 hours and 48 hours the total dosage measured in ovaries nearly tripled, significantly trending upward, and then the study stops. No total percent data is available for bone marrow, but it’s lipid concentration is also trending up at 48 hours.
Any amount of synthetic mRNA that begins self-generating COVID-19 spike proteins in a stem cell or germ cell carries sizable potential for harm.
Why is the following table from the Pfizer biodistribution study so commonly brushed aside by “reputable experts” and regulators?


The EMA claimed no alarm as they simultaneously state in regard to the biodistribution study (they do not release the study itself), “Over 48 hours, distribution was mainly observed to liver, adrenal glands, spleen and ovaries, with maximum concentrations observed at 8-48 hours post-dose.” Note again, the study stops at 48 hours. The toxicity and fertility studies (in animals) they subsequently reference have not been released in full. Here is a chart made of the Pfizer source data (above):
I have seen many attempts to desensitize us to these findings and potential implications, but I have seen zero attempts to validate safety of this concerning biodistribution with anything scientific. Derek Lowe, in a pacifying May 4, 2021 piece in Science (timed perfectly to comfort during “peak jab season” in the USA) entitled “Spike Protein Behavior,” states with regards to the biodistribution study,
The great majority of the radioactivity stays in and around the injection site. In the first hours, there's also some circulating in the plasma. But almost all of that ended up in the liver, and no other tissue was much over 1% of the total.
Ok, but 1% of total dose, or any dose, may be terribly dangerous, especially if in sensitive organs and cell types, like germ cells, bone, spinal cord, gut, and marrow. Note these measurements are snapshots in time from a single injection of 50 micrograms and not cumulative measurements of the dosage. And just as importantly, people are now being offered a lifetime of annual injections. We assumed and studied the primary series as a once-and-done routine—remember that we assumed the vaccine would be effective. Never did we consider or evaluate the cumulative impact (and/or build-up) of mRNA and spike protein in bone, marrow, brain, spinal cord, gut, and so on from repeated dosing every few months.
And what of my metric above looking at the mean lipid concentration in organs/marrow at later time periods relative to the injection site at early time periods, which are quite high, and still trending up at the end of the 48-hr study?
Your regulators have no interest in studying this, and they will approve your next boost without evaluation.
Industry-expert Sasha Latypova claims:
“The only toxicology study that was performed with both the correct version of the vaccine candidate and in compliance with GLP was the repeat dose toxicity study # 20GR142 [this is a primary reference regarding toxicity in the EMA report above]. The full report of this study is not made available. The manufacturer’s own description of the results indicates that the animals experienced appetite loss and weight loss, had fever, had clinical pathology and laboratory parameter changes consistent with inflammation, and not all changes were resolved by the time the study was terminated. Treated animals had enlarged spleens (1.5 times) and lymph nodes. Pathological findings in liver, spleen, bone marrow and lymph nodes were noted but not described in detail, and just waived off by the manufacturer as not significant. There is no way to independently assess these findings.”